By Dr. Elliot Mechanic
Clinicians are routinely presented with critical decisions of selecting the right procedures to best treat the health of patients. Every procedure involves the accurate selection of materials and instruments, and the correct utilization of these tools for ultimate case outcomes.
This article will demonstrate easy, mistake-proof techniques for the predictable accuracy of: single crown impressions, bite registrations, implant impressions, and the registration of a centric relation bite. Creative paths will also be explored for immediate implant stabilization and temporization, and taking easy quad-tray impressions.
Predictable Single Crown Impressions
80% of all crown cases performed are of a single crown. It is a basic, fundamental procedure in dentistry. In order for single crown impressions to be performed correctly the first time every time, predictable procedures are needed to ensure a proper fit with no need for subsequent adjustments.
Common Causes for Impression Errors
Many dentists are perplexed about the many causes of improper impressions. Prior to sending the case to the lab, everything is precisely lined up on the articulator – the occlusion and marginal ridges are perfect, and everything looks correct. The lab then sends it back, it’s placed in the patient’s mouth, and the crown is high or some other unexplainable mistake has occurred. By default, many dentists are quick to blame the lab.
Some common errors can be easily avoided in order to ensure a properly prepared impression to help eliminate ongoing crown adjustments:
Type of Stone – most dentists take a high-quality silicone impression of prepared teeth. Yet, many times, the counter-model is then poured with yellow lab stone, a very inexpensive material with a high co-efficient of expansion. The result is a quality model opposed with a totally distorted model due to the inaccurate stone.
All models should be poured using a low-expansion stone. By using a low expansion material, models are more precise and adjustments will greatly decrease.
Improper Mixing and Pouring of Stone – another common cause of impression errors is that manufacturer directions are not properly followed when mixing and pouring the stone, leading to unwanted expansion and impression inaccuracies.
Exact weights and proportions of water and powder are critical for optimum results. Manufacturer instructions are precisely written for users to closely follow for proper material usage.
Plastic Impression Trays – when placed in the patient’s mouth, plastic impression trays naturally contort which, in turn, distorts the impression material. The material and tray are then further compromised upon removal of the tray, and further damage is inflicted by vibration when the model is poured in the lab.
The use of non-flexing metal impression trays can eliminate many of the errors caused by the use of plastic trays.
Improper Alignment – if the impression tray is not placed in straight – in alignment with the axis of the tooth – there is a high chance of pull and distortion to the impression.
Taking Precise Impressions
Choose the Right Impression Tray – many times, impression trays are used that are too small, impinging on the gingiva bone and preventing proper seating of the impression.
The right impression tray will provide optimum impression seating. A metal impression tray with basic caulk rim locks are ideal to ensure that the tray fits passively in the patient’s mouth without bending or distortion.
Retract and Control Bleeding – there are many different ways to retract and control bleeding. Cord or gingival retraction pastes can be used. If tissue is bleeding, do not take the impression. Ensuring a blood-free field will offer a clear view of margins. All margins should be visible everywhere around the tooth in order for the impression to be created without any undercuts or distortions.
Use Appropriate Impression Materials Dependent on Procedure – different impression materials are specifically designed to address particular needs of the procedure being performed.
Non-Flexing Metal Impression Trays are Critical – because plastic impression trays are flexible, they can cause distortion and inaccuracies that result ill-fitted impressions, adjustments and re-makes.
Taking the Impression
Once the impression is ready to be taken, a low-viscosity light-body material is used to infiltrate into the crevices of the preparation. The firmer heavy-body material displaces the low-viscosity light-body material into the fine crevices at the margins creating a sharp, detailed impression.
Using the Honigum family of products (DMG) Honigum Quad Fast offers a quick 3-minute set. If something firmer is required, Honigum Heavy is an even thicker material that will really accelerate the infiltration of the light-body material.
Honigum materials are mixed with the simple press of a button using the MixStar eMotion machine that eliminates any possible user error. A catalyst and a base are included. With no variation in mixing, consistent results are achieved every single time.
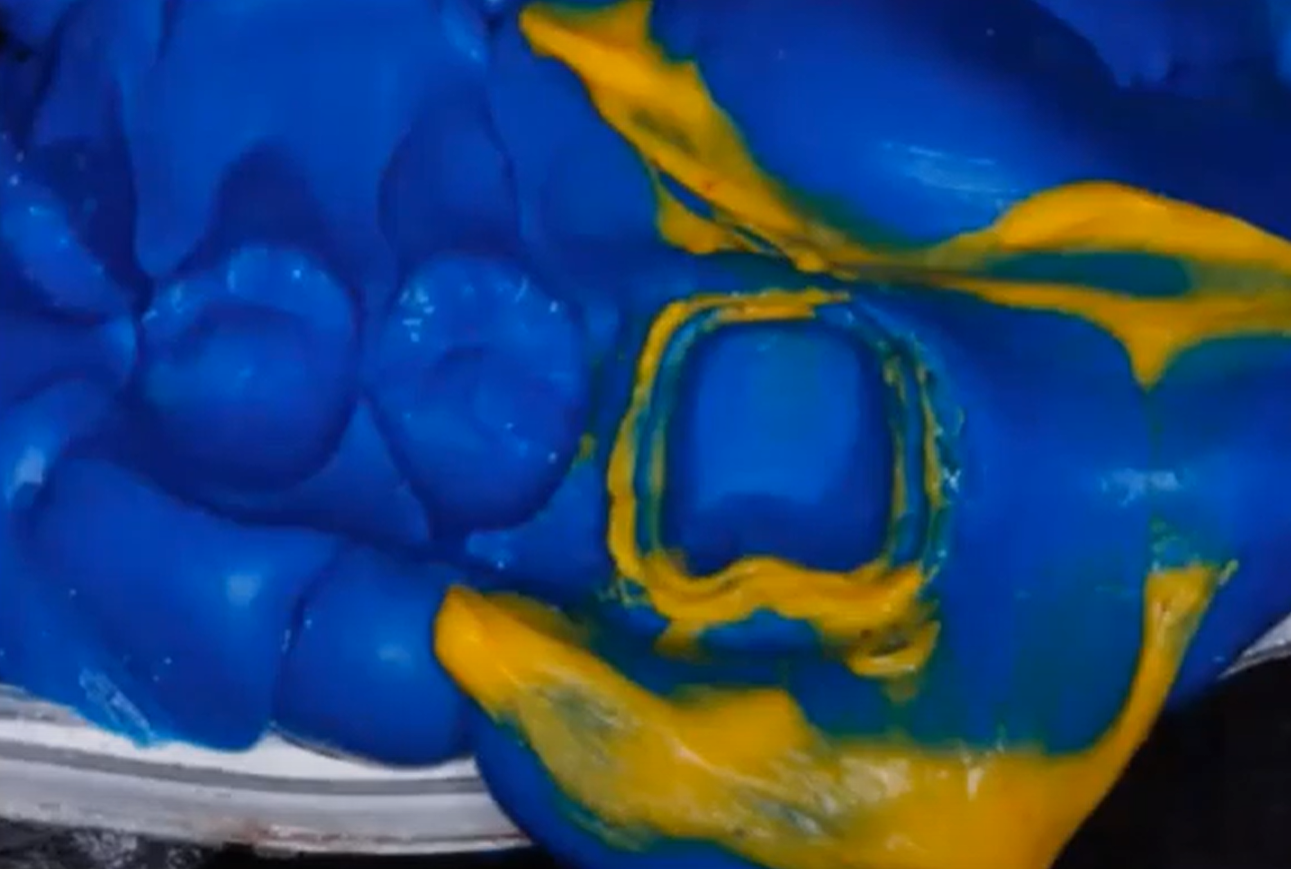
A minimal amount of the heavy-body material is then placed into the quad tray. Because of the ultra thickness of Honigum Quad Fast, there is no chance of it running or sliding off of the quad tray.
If a first molar is prepared, the light-body material is then applied. For a lower tooth, the quad tray is pushed down with a bit of pressure to intrude on the tooth.
The patient then bites down on the quad tray, and the silicone material guides the bite accurately into place. Any inaccuracies in the quad tray impression are virtually impossible using this technique. The result is an extremely accurate margin (Figure 1).
Many dental professionals find quad trays difficult to use. However, these difficulties and resulting errors are typically a result of an improper patient bite and, many times, the dentist is unaware of how the patient is biting. By creating a bite key, all of these variables are eliminated.
Bite Registration
LuxaBite (DMG) is an acrylic-based bite registration material that comes in a standard 10:1 gun. Catalysts and base are included, and it is dispensed out of mixing tips for mixing consistency. When doing a LuxaBite bite registration, always use cheek retractors in order to clearly determine if the back teeth are occluded. In addition, only apply the bite registration to the prepared teeth.
Bite Registration for Final Provisionals
One of the most important tools to help eliminate overall mistakes and variables in practice is an operatory timer. Exact instructions and timing must be followed with every material and procedure for ideal results.
Discussed here is how to take an accurate bite registration using the conventional LuxaBite technique for a full mouth case.
Taking A Centric Relation Bite Record
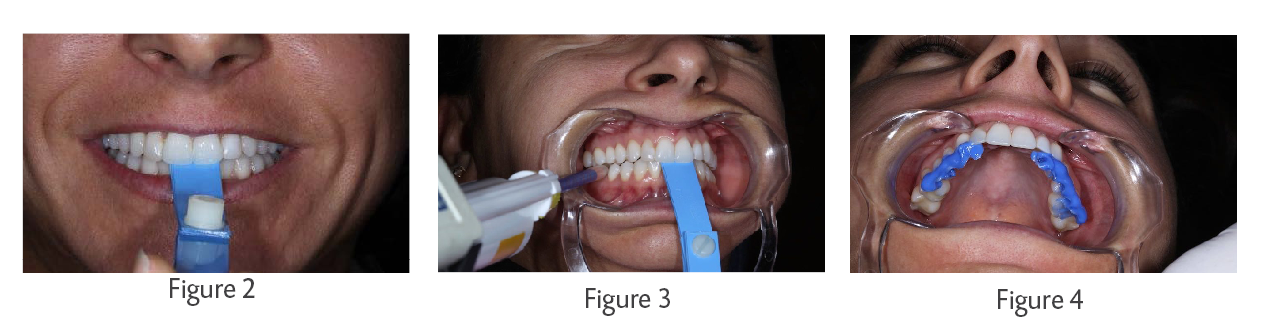
A leaf gauge is very similar to a bite plate. It encompasses 6-8 leafs that are manipulated by the back and forth squeezing motion of the mouth (Figure 2). An opening is created using a 7-8 leaf thickness. LuxaBite is then injected into the small opening created by the centric relation bite registration (Figure 3).
The bite is then locked with LuxaBite. Used bi-laterally (with cheek retractors in place), LuxaBite is also placed on the opposing side. After setting for 2 minutes, the result is an ideal bite registration (Figure 4). The lab can now take the models and lock the bite into the indentations in the LuxaBite.
Implant Impressions
A tried and true way of achieving a secure, accurate implant impression is that of tying the transfers with floss, and then securely bounding them together using a strong acrylic-based material. Using this technique completely inhibits any movement and stabilizes the impression.
Immediate Implant Technique Case
In an unusual case, a 47-year old female presented with a false tooth held in her mouth by a whitening tray. The tooth was extracted one week prior, and the treatment plan suggested by her dentist was an implant. Prior to the extraction, she had simultaneous root canals on all four front teeth many years before.
The crown had failed on the extracted tooth, and the root was rotted inside. Her dentist suggested treating one tooth at a time – extract the one tooth, place the implant, and then if the other teeth failed in the future, the same would be done.
In order to develop a proper treatment plan, an x-ray was suggested to access the full situation.
After taking a panoramic x-ray, it was clear that all four 25-year old root canals were destined to fail.
In addition to the restorative work, simultaneous orthodontic treatment was suggested because there was currently not enough room to replace the lateral with an implant. In addition, the lower bite was collapsed inwards causing added pressure to the front teeth.
An orthodontic scan was done so the patient was able to see the movement and expansion needed to create enough space for the lateral implant.
Deciding to move forward, lower orthodontics were started during the same period as the upper teeth restorations. To ascertain the health of the other anterior teeth, all crowns were removed and, as expected, the teeth were resorbing and decayed, and the cast posts were loose and emitting a bad odor. All teeth were re-temped in anticipation of the implants.
The temporaries were very thinly fabricated as to not cause any opposition with the orthodontic work being done on the lower teeth.
Immediate implants were then placed on two centrals and one of the laterals, and a 5-unit cantilever bridge was created extending from the one canine to the other lateral. A veneer was planned for the front natural canine. Immediate implants were done.
At this point, the teeth were extracted, the implants were placed, and temporary abutments were made for immediate loading.
The three temporary implant abutments were joined together to stabilize the implants and evenly distribute forces on the immediate implants. A platform was then made out of Luxatemp (DMG) for the other temporary – thus creating a temporary over a temporary.
The Luxatemp over Luxatemp is joining everything together and stabilizing the implants. While everything is integrating, the lower orthodontic work is simultaneously being finished.
An impression is taken, and using the color of the prepared teeth, the temporary abutments are placed.
Luxatemp provisionals are created again while everything is healing, and the case is sent to the lab.
In addition, the lower arch is now in line and a final shade matching is done.