Written by Louis Kaufman, DDS, FAGD, MBA
Dental practices and dental patients both seem to be facing increased time and cost pressures, which means that we all need to place a greater premium on efficiency than ever before. One of the keys to optimizing the efficiency – as well as the profitability – of my practice has been to invest in equipment and materials that allow me to perform my bread-and-butter procedures both quickly and reliably. After all, increased speed without reliable outcomes is a sure way to worsen, not improve, your efficiency. One of my bread-and-butter procedures that I perform at least three-to-four times a week is first molar restorations. The ability of my practice to mill our own “same day” crowns has brought us dozens of new patients, such as busy executives who simply do not have the time for a second visit or, elderly patients for whom a second visit is highly inconvenient. It has also helped reduce our costs and enhance our profitability.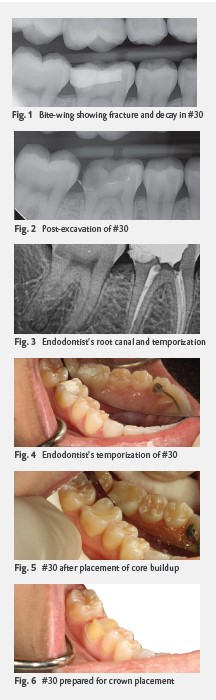
Finding the right manufacturer-partners is essential to fine-tuning your blend of speed and reliability. I have been able to achieve highly predictable outcomes using adhesive, cement and composite materials made by a single manufacturer – DMG – known for the extraordinary amount of research that goes into its product development.
The Case
A 22-year-old female presented having experienced significant pain for several months in tooth #30. Like many patients, she had lived with the pain in hopes that it would eventually resolve itself, but she finally concluded that professional treatment was required. The challenge was clear: I needed to provide not only relief to her immediate pain, but a permanent solution to that pain. I decided to capture all aspects of the case with my 3D scanner system (iTero; Align Technologies). As with any emergency patient, my dental assistants know to capture periapical and bitewing radiographs as well as an introaral photo of the offending tooth. My first step was to achieve profound anesthesia by infiltrating the tooth with an interosseous injection of articaine hydrochloride 4% with epinephrine 1:100,000 (Septocaine; Septodont) through the buccal plate. Next, I isolated the site with an isolation system (Isolite; Zyris), which I used throughout the procedure.
I took an initial X-ray, which revealed a fracture and significant decay (Fig. 1), and then excavated the decay. This allowed me to see that we were near pulp exposure. I took another X-ray (Fig. 2) and temporized the patient with an IRM (intermediate restorative material) sedative filling (IRM ZOE; Dentsply Sirona). I then sent her to the endodontist, who performed a root canal and also gave her an IRM temporization (Figs. 3 and 4). The X-rays provided by the endodontist indicated that he was able to get down to sound dentin.
When the patient returned to my practice a week later, it was the day before she had to fly back to college. Fortunately, my in-office milling system (glidewell.io; Glidewell Dental) would enable me to design, manufacture and place the crown in one visit. I began the procedure by again isolating the site for the entire procedure. I cleaned out the IRM and cleansed the cavity site with an antimicrobial cavity cleanser (FiteBac; Largent Health). For the bonding, I used a dual-cure adhesive (LuxaBond Total Etch; DMG). I use LuxaBond Total Etch for virtually all of my bonding, including cases that involve doing a direct post and core and require the secure bonding of the post into the canal space. After the application of the adhesive, I used a dual-cure composite for the core buildup (LuxaCore Z Dual; DMG), making certain to fill in any undercuts (Fig. 5). I use the LuxaCore Z Dual because it is dual cure, very hard-setting, and exhibits no ditching. Once the buildup was placed, I prepared the tooth for the crown (Fig. 6).
I then used the iTero to scan the tooth, and sent the scan to the glidewell.io. Its design software used AI to mark the margin (Fig. 7), which I then refined. Next, we used the fastdesign.io software to design the crown.
The crown was then milled using zirconia (BruxZir; Glidewell). Once milled, the crown’s sprue (Fig. 8) was removed, and the crown was polished and tried in (Fig. 9). The fit was verified with a bitewing X-ray (Fig. 10). After try-in, I cleaned the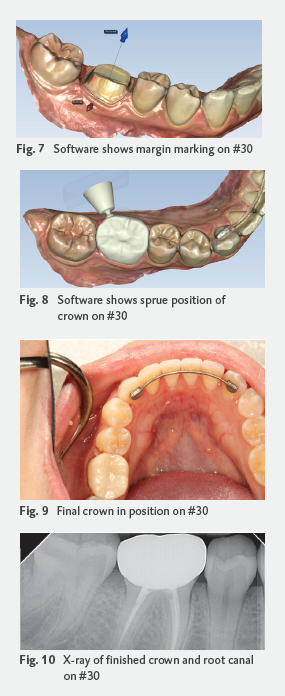 crown using a universal cleaning paste (IvoClean; Ivoclar), and permanently bonded the crown using a self-adhesive cement (PermaCem 2.0; DMG).
crown using a universal cleaning paste (IvoClean; Ivoclar), and permanently bonded the crown using a self-adhesive cement (PermaCem 2.0; DMG).
About six weeks later, the patient reported that she had experienced no pain since the procedure and was very pleased with the fit and feel of the crown.
Conclusion
By definition, bread-and-butter procedures are essential to any practice’s success. Having the optimal techniques, equipment and materials are essential to your ability to perform those procedures with the ideal balance of efficiency and reliability that will maximize both patient satisfaction and practice profitability.
About the Author
Dr. Louis Kaufman is a General Dentist in Chicago, Illinois. Dentistry is constantly evolving, and leading change is Dr. Kaufman’s core mission. He earned his DDS from the University of Illinois at Chicago, earned his Fellowship in the Academy of General Dentistry and is a member of the Alpha Omega International Dental Society. He holds a MBA in Executive Management from DePaul University and a BS in Computer Science with a BA in Marketing and Finance from Kendall College. The owner of a 70-year-old practice started by his father, Dr. Kaufman serves on the advisory board of numerous dental manufacturers and educates clinicians across the globe on a wide range of topics through lectures and articles. An administrator with Smile Source Chicago, Dr. Kaufman is a member of numerous professional organizations, including the ADA, AGD, AACD, AADSM, ICOI and AAID. Dr. Kaufman has discovered ways to measurably improve the patient experience, grow practices and increase revenue. He has learned how to improve processes and leverage technologies to overcome clinicians’ most common challenges. It is these skills that he will share with you in his teachings.